History
Because a firm diagnosis of thromboangiitis obliterans (TAO; also referred to as Buerger disease), is difficult to establish, a number of different diagnostic criteria have been proposed. [7] In 1990, Olin et al asserted that the following criteria must be met for the diagnosis to be made with reasonable certainty [8] :
-
Age younger than 45 years
-
Current (or recent) history of tobacco use
-
Presence of distal extremity ischemia (indicated by claudication, pain at rest, ischemic ulcers, or gangrene) documented by noninvasive vascular testing
-
Exclusion of autoimmune diseases, hypercoagulable states, and diabetes mellitus by laboratory tests
-
Exclusion of a proximal source of atheroemboli by echocardiography and arteriography
-
Consistent arteriographic findings in the clinically involved and noninvolved limbs
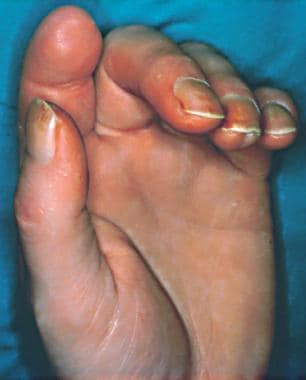
Most patients with TAO (70-80%) present with distal ischemic rest pain or ischemic ulcerations on the toes, feet, or fingers (see the image below). [9, 10] Progression of the disease may lead to involvement of more proximal arteries, but involvement of large arteries is unusual.
 Feet of patient with thromboangiitis obliterans (Buerger disease). Note ischemic ulcers on distal portion of left great, second, and fifth toes. Although patient's right foot is normal in gross appearance, angiography demonstrated compromised arterial flow to both feet.
Feet of patient with thromboangiitis obliterans (Buerger disease). Note ischemic ulcers on distal portion of left great, second, and fifth toes. Although patient's right foot is normal in gross appearance, angiography demonstrated compromised arterial flow to both feet.
Patients may also present with claudication of the feet, legs, hands, or arms and often describe experiencing the Raynaud phenomenon (a pathologic vasospastic process involving pain, paresthesias, and color changes of the digits of the hands and feet in response to cold or anxiety).
Patients who seek medical attention late in the course of their disease may present with foot infections and, occasionally, with florid sepsis.
Physical Examination
Patients with TAO can develop painful ulcerations (see the image below) or frank gangrene of the digits. The hands and feet of patients with the disease are usually cool and mildly edematous.
 Tobacco smoke stains on male patient's fingers suggest diagnosis of thromboangiitis obliterans (Buerger disease). Patient presented with small, painful ulcers on tips of thumb and ring finger.
Tobacco smoke stains on male patient's fingers suggest diagnosis of thromboangiitis obliterans (Buerger disease). Patient presented with small, painful ulcers on tips of thumb and ring finger.
Superficial thrombophlebitis (often migratory) occurs in almost half of patients with TAO (see the image below). Paresthesias (numbness, tingling, burning, hypoesthesia) of the feet and hands and impaired distal pulses in the presence of normal proximal pulses are usually found in patients with severe disease. More than 80% of patients present with involvement of three or four limbs.
 Superficial thrombophlebitis of great toe in patient with thromboangiitis obliterans (Buerger disease).
Superficial thrombophlebitis of great toe in patient with thromboangiitis obliterans (Buerger disease).
In 1996, Papa et al proposed a point-scoring system to support or contest the diagnosis of TAO on the basis of the following criteria [11] :
-
Distal extremity (feet, toes, hands, or fingers) involvement
-
Onset before age 45 years
-
Tobacco use
-
Exclusion of atherosclerosis or proximal source of emboli
-
Absence of a hypercoagulable state
-
Absence of definable arteritis (eg, progressive systemic sclerosis or giant-cell arteritis)
-
Classic arteriographic findings
-
Involvement of digital arteries of finger or toes
-
Segmental involvement (ie, “skip areas”)
-
“Corkscrew collaterals”
-
No atherosclerotic changes
-
Classic histopathologic findings
-
Inflammatory cellular infiltrate within thrombus
-
Intact internal elastic lamina
-
Involvement of surrounding venous tissues
The scoring system is applied as indicated in Table 1 and Table 2 below.
Table 1. Scoring System for Diagnosis of Thromboangiitis Obliterans [11] (Open Table in a new window)
Positive Criterion |
Positive Points |
||
Age at onset |
< 30 y (+2) 30-40 y (+1) |
||
Foot intermittent claudication |
Present (+2) By history only (+1) |
||
Upper extremity |
Symptomatic (+2) Asymptomatic (+1) |
||
Migrating superficial thrombophlebitis |
Present (+2) By history only (+1) |
||
Raynaud phenomenon |
Present (+2) By history only (+1) |
||
Angiography; biopsy |
If typical, both (+2) Either(+1) |
||
Negative Criterion |
Negative Points |
||
Age at onset |
45-50 y (−1) >50 y (−2) |
||
Sex; smoking |
Female (−1) Nonsmoker (−2) |
||
Location |
Single limb (−1) No lower extremity involved (−2) |
||
Absent pulses |
Brachial (−1) Femoral (−2) |
||
Arteriosclerosis, diabetes, hypertension, hyperlipidemia |
Discovered 5.1-10 y after diagnosis (−1) Discovered 2.1-5 y later (−2) |
||
Table 2. Numerical Scores Defining Probability of Diagnosis of Thromboangiitis Obliterans (Open Table in a new window)
Score |
Probability of Diagnosis |
0-1 |
Diagnosis excluded |
2-3 |
Diagnosis suspected (low probability) |
4-5 |
Diagnosis probable (medium probability) |
≥6 |
Diagnosis definite (high probability) |
Complications
Potential complications of TAO include the following:
-
Ulcerations
-
Gangrene
-
Infection
-
Need for amputation
-
Rare occlusion of coronary, renal, splenic, or mesenteric arteries
-
Feet of patient with thromboangiitis obliterans (Buerger disease). Note ischemic ulcers on distal portion of left great, second, and fifth toes. Although patient's right foot is normal in gross appearance, angiography demonstrated compromised arterial flow to both feet.
-
Superficial thrombophlebitis of great toe in patient with thromboangiitis obliterans (Buerger disease).
-
Tobacco smoke stains on male patient's fingers suggest diagnosis of thromboangiitis obliterans (Buerger disease). Patient presented with small, painful ulcers on tips of thumb and ring finger.
-
Lower-extremity arteriogram of peroneal and tibial arteries of patient with thromboangiitis obliterans (Buerger disease) demonstrates classic findings of multiple small and medium-sized arterial occlusions with formation of compensatory "corkscrew collaterals."
Tables
Positive Criterion |
Positive Points |
||
Age at onset |
< 30 y (+2) 30-40 y (+1) |
||
Foot intermittent claudication |
Present (+2) By history only (+1) |
||
Upper extremity |
Symptomatic (+2) Asymptomatic (+1) |
||
Migrating superficial thrombophlebitis |
Present (+2) By history only (+1) |
||
Raynaud phenomenon |
Present (+2) By history only (+1) |
||
Angiography; biopsy |
If typical, both (+2) Either(+1) |
||
Negative Criterion |
Negative Points |
||
Age at onset |
45-50 y (−1) >50 y (−2) |
||
Sex; smoking |
Female (−1) Nonsmoker (−2) |
||
Location |
Single limb (−1) No lower extremity involved (−2) |
||
Absent pulses |
Brachial (−1) Femoral (−2) |
||
Arteriosclerosis, diabetes, hypertension, hyperlipidemia |
Discovered 5.1-10 y after diagnosis (−1) Discovered 2.1-5 y later (−2) |
||
Score |
Probability of Diagnosis |
0-1 |
Diagnosis excluded |
2-3 |
Diagnosis suspected (low probability) |
4-5 |
Diagnosis probable (medium probability) |
≥6 |
Diagnosis definite (high probability) |







