
Abstract
To evaluate the percentage of hypertensive patients who could achieve target blood pressure (TBP) according to the guidelines in the context of recommended measures and the factors responsible for failure. A total of 589 hypertensive patients (59.0% female; mean age: 57.7±10.4 years) were assessed twice for TBP achievement based on 2007 ESH/ESC guidelines and the investigators’ view, in addition to the recommended measures and possible causes of failure in hypertension management in this national multi-center (n=99), non-interventional observational study. Only 29.5% of the patients at the first visit and 46.8% at the second visit achieved the TBP levels specified by the guidelines. However, the investigators’ evaluation indicated a higher achievement rate at the first (43.5%) as well as the second (69.1%) visit when compared with the guideline-based assessments (P<0.001). The primary reasons identified by the investigators for the failure to reach TBP were non-compliance with dietary recommendations (61.6%) at the first visit and non-compliance with treatment (63.92%) at the second visit. Recommendations for lifestyle were the most commonly identified treatment plan by the investigators at both visits (62.9% and 66.1%, respectively). Although more patients achieved the TBP levels specified by the guidelines for the second visit compared with the first, effective blood pressure control was achieved only in 29.5% of our patients. Interestingly, the investigators had a more optimistic view about their patients’ control of hypertension, which may have contributed to a poor achievement of TBP.
Similar content being viewed by others

Introduction
Owing to a very high lifetime risk of development, the prevention and management of hypertension is considered to be among the major public health challenges.1
With an estimated worldwide prevalence of approximately 1 billion individuals and approximately 7.1 million deaths per year that can be attributed to hypertension, primary prevention measures should be introduced to minimize its causal factors in the population.1, 2 In addition, the World Health Organization (WHO) reports that a suboptimal blood pressure (BP) (systolic BP (SBP) >115 mm Hg) is responsible for 62% of cerebrovascular disease and for 49% of ischemic heart disease, with little variation by sex.1
Despite encouraging data on the benefits of strict BP control in diminishing the cardiovascular risk reported by several clinical trials, the achievement of BP control continues to remain unsatisfactory in many areas of the world.3, 4
Various organizations worldwide collaborate on hypertension as a crucial health problem and several guidelines are available for the diagnosis, treatment and follow-up of hypertension. Among these guidelines, ‘The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High blood Pressure’ (JNC-7 Report) by the American National Heart, Lung and Blood Institute1 and the European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension (ESC/ESH guidelines) each have considerable importance.5 As indicated in the JNC-7 report, undiagnosed, untreated and uncontrolled hypertension places a substantial strain on the healthcare delivery system. Hence, suboptimal BP is the number one attributable risk factor for death throughout the world, with current control rates for hypertension that are far from acceptable.1, 2
According to the 2007 ESC/ESH guidelines,5 the main objectives of the evaluation of hypertensive patients are to assess their lifestyle and to identify other cardiovascular risk factors or concomitant disorders that may affect the prognosis and guide treatment, to reveal the identifiable causes of high BP and to assess the presence or absence of target organ damage and cardiovascular disease (CVD). In accordance with the primary goal of therapy in patients with hypertension, including a maximum reduction in the long-term total risk of CVD through the treatment of elevated BP and reducing or treating the associated reversible risk factors, once antihypertensive drug therapy is initiated, most patients should return for follow-up and the adjustment of medications at monthly intervals or until the BP goal is reached.1 Therefore, the present study was designed to evaluate the percentage of hypertensive patients who could achieve target BP (TBP) values according to the 2007 ESH/ESC guidelines, and to identify factors associated with the failure to reach TBP as well as recommended measures to be taken.
Methods
Study population
According to the study's flowchart presented in Figure 1, 589 of the 603 enrolled patients were considered to be eligible in terms of age (26–84 years; median age: 58 for females and 57 for males) and who were previously diagnosed with essential hypertension and were receiving antihypertensive medications. Other eligibility criteria were the availability of previous laboratory evaluations for the assessment of risk factors within the past 3 months and attending a routine visit to their physicians at study centers (n=99, internal medicine and cardiology clinics) in this national multi-center, non-interventional observational study. Data collection was performed between January and March 2009 at two different time points (at the time of enrollment (visit 1; mean age: 57.7±10.4 years) and 2 months later (visit 2; mean age: 56.7±10.3 years)). Patients with either a known or a suspected diagnosis of secondary hypertension who were currently hospitalized or planned to be hospitalized during the study period and who were enrolled for another study were excluded from this study.

Flow chart of the study concerning the disposition of patients.
In this registry study, 103 sites were selected initially from the hospitals treating hypertension, but a total of 99 provided data concerning 603 patients. Each site was instructed to invite hypertensive patients who had attended the clinic and fulfilled the above-listed selection criteria to participate in the study. Of the 603 enrolled patients, 589 had evaluable data. During the patient enrollment period of 2 months, six patients from each center were planned to be enrolled in the study. Participating sites/investigators were asked to enroll the second hypertensive patient who visited the physician for routine control on each working day. This patient selection method was offered to prevent a potential selection bias that might lead to a nonresponse bias resulting from the respondents differing in meaningful ways from the nonrespondents. The ESC/ESH 2007 guidelines were referred to by the internists/cardiologists who participated in this study for decisions about the appropriate actions for achieving better BP control.
Written informed consent was obtained from each subject following a detailed explanation of the objectives and protocol of the study, which was conducted in accordance with the ethical principles stated in the ‘Declaration of Helsinki’ and approved by the institutional ethics committee.
Assessments performed at the initial visits (visit 1) and at visits during the second month (visit 2)
Patient demographics (gender and age), anthropometric measurements, medical history related to the concomitant diseases, risk factors and antihypertensive treatments were recorded. The percentage of treated hypertensive patients who did not achieve a TBP both according to the guidelines and the investigator's opinion was calculated. The investigator's evaluation concerning the TBP achievement was on the basis of their response to a specific question in the case report form: ‘Did your patient achieve TBP?’ Another evaluation was performed by the statistician, with a data set analysis based on BP values specified by the guidelines when the BP values of patients were recorded by the physician. Therefore, for some patients, the investigator's opinion was available, but data for the guideline-based evaluation of TBP achievement were lacking because of the absence of recorded BP values.
According to the guidelines, the factors influencing prognosis are defined as risk factors, such as gender, age and smoking status, subclinical organ damage, diabetes mellitus (DM), and other concomitant diseases. Data were collected for subclinical organ damage in the patient population based on previous recordings for echocardiography, carotid Doppler examinations, ocular fundus evaluations and serum creatinine levels. The detection of microalbuminuria in spot urine samples was also recorded if available.
In accordance with the non-interventional observational character of the study, the treatment decision was left to the discretion of the physician and documented in the case report form (antihypertensive agent class and dosages). Considering alternative treatments for those patients with uncontrolled BP, their current medication(s) was also at the discretion of the physician, either by prescribing a new drug, adding another drug class or increasing the dosage of the existing medication(s). For some data points, there were missing/incomplete data that were not queried during the data management period because this study was planned as a real-time observational registry study.
BP measurement was performed by trained physicians in accordance with the standard technique described in JNC-7 Report by the American National Heart, Lung and Blood Institute,1 and the 2007 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension (ESC/ESH guidelines). High BP was considered to be a SBP >140 mm Hg and a diastolic BP (DBP) >90 mm Hg.1, 5 At the time of enrollment, the patients were graded as TBP achieved or not achieved according to a final BP measurement. The investigators were instructed to invite patients who had not achieved TBP levels (n=333) for a second visit 2 months after the initial visit. These patients were also asked to complete a BP-recording diary for 2 months and bring it to the second visit, during which the factors associated with the failure to reach TBP as well as the achievement rate and measures taken to reach a TBP were re-evaluated. Finally, the investigators performed a BP recording in their office and also transferred the last available BP recording from the patient's diary to the patient's case report form during the second visit, to calculate the mean BP based on values obtained from the office recording during the second visit and from the patient's diary during the period between visits. The opinions of the investigators about the possible causes of failing to reach TBP levels and the recommended measures for achieving a TBP as well as their estimates of the length of time required to meet the target in the near future were also questioned during the study visits.
The TBP was considered to be ⩽130 mm Hg for SBP and/or ⩽80 mm Hg for DBP in patients with DM or with high/very high CV risk factors (myocardial infarction, CVD, chronic kidney disease, proteinuria) and ⩽140 mm Hg and/or ⩽90 mm Hg for the remainder of the patients.
Statistical analysis
This study hypothesized that the percentage of patients reaching TBP levels would be approximately 30% or less with a 4% error within a 95% confidence interval with a sample size calculated at a minimum of 492 patients. The calculation of the rate of patients reaching TBP levels does not require any patient follow-up, thus the initial BP levels for all patients would be satisfactory. However, as TBP levels could be evaluated more accurately according to the risk factors, a complete profile of clinical and laboratory determinants was planned to be recorded at the second visit 2 months later. In cases of missing data, a dropout rate of 15–20% was proposed, thus increasing the sample size to 600 patients. However, of the 603 patients enrolled, 589 were considered to be eligible, and because of missing data, the total number did not reach 589 for some of the parameters collected.
Statistical analysis was performed using Stata Data Analysis and Statistical Software (Version 10, StataCorp LP,College Station, TX, USA). Inter-group comparisons were performed using χ2 or Fisher exact tests for categorical data and using Mann–Whitney U-test or Student's t-test for numerical data. Comparisons for the perceptions of physicians vs. guideline requirements were performed using a two-sample proportion test. Data were expressed as ‘mean (s.d.)’, percent (%) and 95% confidence interval. A value of P<0.05 was considered to be statistically significant.
Results
Basic clinical features
Data for anthropometric parameters were available for 294 patients (Table 1). In male patients (n=81; 27.6%), the waist circumference was >102 cm and in females (n=213; 72.5%) it was >88 cm. The body mass index (BMI) was calculated for all patients and classified according to the WHO Classification,6 and the results revealed that 269 (48.3%) of the patients were obese (Class I, II and III). The median (min–max) duration of hypertension was 62 (1–480) months and the mean (s.d.) levels of systolic (174.5 (23.0) mm Hg) and diastolic (101.7 (11.6) mm Hg) BP levels at the time of initial diagnosis were high. Roughly one-third of the patient population in this study was diabetic 170 (28.9%), and 213 (39.6%) patients had a positive family history of CVD.
TBP achievement status at visit 1
Referring to the guidelines, the data collected at visit 1 indicated that, among the 562 patients, only 29.5% (n=166) achieved TBP levels (Table 1). When the percentage of TBP achievement was evaluated according to the investigators’ point of view, it indicated a higher achievement rate, including 256 patients (43.5%) (Table 1, Figure 2). When compared with the investigators’ view, the percentage of patients who failed to achieve a TBP at visit 1 and succeeded in achieving a TBP at visit 2 was determined to be significantly higher according to a guideline-based evaluation (P<0.01 for each; Figure 2). In addition, a significantly higher percentage of patients achieved the TBP in visit 2 for both the guideline-based evaluation and the investigators’ view (P<0.01 for each; Figure 2).When analyzed on the basis of target SBP and DBP values, 35.1% (n=196) of the patient population achieved the target systolic level, whereas 37.8% (n=211) achieved the target DBP level.

Target blood pressure (TBP) achievement status of the patients determined with respect to the guidelines and the investigators’ view. *P<0.01; compared with the percentage of patients determined according to the investigators’ view in the same population. +P<0.01; compared with the percentage of patients who failed to achieve a TBP according to the guidelines in visit 1. qP<0.01; compared with the percentage of patients who failed to achieve a TBP according to the investigators’ view in visit 1.
There were 170 diabetic patients among the complete data set at visit 1. Only 24 (14.1%) of them were at their TBP levels (Table 1). On the other hand, the BP recordings of 142 (36.2%) non-diabetic patients were at the targeted levels (Table 1).
TBP achievement was also evaluated by age groups vs. BP groupings as defined by the guidelines. Patients in the age group of 40–49 years had the highest ratio of failure (83.2%) for achieving the TBP levels, whereas patients in the 50–59-year-old group were the most successful in reaching the goal (36.3%).
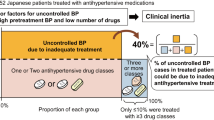
The evaluation of antihypertensive treatment during visit 1 revealed that 267 patients (46.1%) received mono-therapy and 215 (36.9%) received a two-drug combination, whereas in 14.9 % cases (n=90), more than three antihypertensive medications were prescribed, as shown in Table 2. The most frequently prescribed pharmaco-therapeutical groups of antihypertensive medications were angiotensin receptor blockers (7.1%) and angiotensin receptor blocker plus diuretic combinations (16.9%) (Table 2).
Reasons for failure and recommended measures for reaching TBP levels according to the investigators at visit 1
From the investigators’ point of view, 205 (61.6%) (Table 3) patients were unable to achieve TBP levels because of non-compliance with the dietary recommendations, whereas insufficient doses of the prescribed antihypertensive treatment were implicated for 38.7% (n=129) of them.
Re-recommendations on life style changes (66.1%, n=205), training of the patient (54.0%, n=180) and the addition of a new antihypertensive drug to the treatment were the main treatment plans identified by the investigators for patients who failed to achieve TBP levels.
The investigator's estimation of the time required to achieve TBP levels by the treatment plans after the first visit was 1–4 weeks for 206 (63.8%) of the 333 patients who were not successful in achieving TBP levels during enrollment.
Factors influencing prognosis (risk factors, organ damage, DM and other concomitant diseases)
The risk factors evaluated for the prognosis were gender, age and smoking status. An analysis of the data showed that for female patients, there was a statistically significant positive relationship between age and the achievement of TBP (for male patients: P=0.212 and for female patients: P=0.037). Both gender groups showed similar patterns of hypertensive history, including duration of hypertension, SBP and DBP values at the time of diagnosis and study visits (Table 4). It was observed that 95 (16.3%) of the 589 recorded patients were current smokers, 127 (21.8%) were former smokers and 362 (62.0%) were non-smokers. The percentage of active smokers was 24.4% (n=58) among males and 10.5% (n=36) among females (Table 4). The data set for 589 patients showed that 351 (59.6%) patients were previously evaluated by echocardiography for left ventricular hypertrophy. Data showed that 169 patients (48.8%) had left ventricular hypertrophy, as demonstrated in Table 1.
The carotid Doppler examination rate was low (7.1%); however, the data collected showed that 42.1% of the examined patients had thickening of the carotid wall and 27.0% had carotid plaques. An ocular fundus examination was performed for 21.2% of patients and indicated a high rate of hypertensive retinopathy (45.6%).
Serum creatinine evaluations were available for most of the patients (n=520), with a mean creatinine level of 0.9±0.3 mg dl−1. For a minority of patients (n=72), the average microalbuminuria in the spot urine was determined to be 102.8±215.6 mg.
An evaluation for dyslipidemia revealed that 51.0% of the patients had total cholesterol values greater than 200 mg dl−1. Approximately one in every two patients had low-density lipoprotein cholesterol levels higher than 130 mg dl−1 (Table 1).
The existence of cardiovascular comorbidities, including cerebrovascular disease, heart disease, renal dysfunction and peripheral vascular disease, were observed in 172 cases (29.2%). There was a statistically significant relationship between increasing age and the rates of heart failure (P=0.012), myocardial infarction (P=0.011), peripheral vascular disease (P=0.028) and concurrent revascularization (P=0.004).
Patients with cardiovascular morbidity were evaluated for achieving TBP levels; however, no significant relationship was noted. This finding was most likely because of the low number of patients with those medical conditions among the selected patient population of the study.
TBP achievement status at visit 2
A total of 307 patients (92.0% of the invited patients) attended the second visit. The BP recordings performed at the physician's office were significantly higher than the patients’ home recordings, both for systolic (130.0 (15.7) vs. 134.4 (16.9) mm Hg) and diastolic (78.8 (10.1) vs. 82.7 (10.0) mm Hg) levels (P<0.001 for each).
According to the investigators, 69.1% of the patients (n=210) reached TBP levels, although an evaluation of the database revealed that only 46.8% of all patients attending the second visit were able to achieve BP control according to the levels specified by the guidelines (Table 1; Figure 2). Similar to the enrollment visit, the rate of TBP achievement was found to be lower (11.0%) among diabetic patients compared with non-diabetics (60.7%) (Table 1).
The evaluation of SBP and DBP levels revealed that 11.5% (n=35) of all cases could not achieve systolic TBP levels and 3.3% (n=10) could not achieve diastolic TBP values.
Reasons for failure and recommended measures for reaching TBP levels according to the investigators at visit 2
As shown in Table 3, non-compliance with the treatment (63.9%) was identified by the investigators at visit 2 as the leading cause of failure in achieving TBP levels. Recommendations for lifestyle (62.9%) and patient training (53.6%) were the investigators’ most common suggestions for their patients to reach TBP in a short term (1–4 weeks according to 68.7% of the investigators).
Discussion
Guidelines recommend that the management of hypertension begin with lifestyle modifications, and if the BP goal is not achieved, five groups of antihypertensive medication (that is, angiotensin converting enzyme inhibitors, angiotensin receptor blockers, beta-blockers and calcium channel blockers) can be used as initial or maintenance therapy for most patients.5 According to our findings, monotherapy in 46.0% of the enrolled patients and a two-drug combination in 36.8% of patients were the selected antihypertensive treatments. Furthermore, angiotensin receptor blocker and a diuretic combination were the most frequently prescribed medications (16.9%), in accordance with the guidelines. However, TBP achievement was evident only in one-third of the study population.
On the basis of the guidelines, one-third (29.5%) of the overall population at visit 1 and almost half of the population (46.8%) at visit 2 achieved TBP levels, whereas the exclusion of diabetics revealed slightly better achievement rates (36.2%) because the TBP was achieved by only 14% of the diabetic population. The BP control rate obtained in our study population was in agreement with the previously reported effective BP control in only one-third of US patients with hypertension, despite multiple treatment options available for hypertension.6
Interestingly, when the percentage of TBP achievement was evaluated from the investigators’ point of view, higher rates were identified at both visits (43.5 and 69.1%) compared with the guideline-based analysis. In this regard, database-derived results indicate that investigators seem to have a more optimistic perspective of the understanding of achieving TBP levels for their patients, on the grounds of control of hypertension for the protocol population. Investigators may assume that target levels were achieved; however, the BP recordings do not meet the criteria set by the 2007 ESC/ESH guidelines, as evident in 14.0% of our patients during the first visit and 22.6% of our patients during the second visit. Furthermore, during both visits, most of the investigators expected a quicker response rate to their treatment options as shown in their responses that their patients will reach TBP levels in 1–4 weeks.
Likewise, in the Supporting Hypertension Awareness and Research Europe-wide (SHARE) physician survey that aimed to qualify the key challenges facing physicians when they are trying to get patients to a BP goal, it was reported that overall, 95.0% and 90.1% of the physicians felt that patients’ SBP and BP, respectively, needed to be higher than the guideline's recommended goal levels before taking immediate action. In this regard, a clinical hesitation in reducing elevated BP to goal levels puts patients at an increased cardiovascular risk and contributes to the substantial health and economic burden associated with uncontrolled BP.7
The adoption of healthy lifestyles by all persons is critical for the prevention of high BP and is an indispensable part of the management of those with hypertension.8 Failure to prescribe lifestyle modifications, adequate antihypertensive drug doses or appropriate drug combinations, in addition to unsatisfactory patient compliance5, 9 may result in inadequate BP control.1
In this respect, in a recent practice-based, cross-sectional, observational, mailed survey conducted on patients with type 2 diabetes in three eastern provinces in Canada, 54.0% of patients were reported to be at target for both systolic and diastolic pressures. Moreover, patients who reported eating food low in salt had higher odds of reaching TBP, whereas patients reporting a low adherence to their medication regimen had lower odds of reaching a TBP.10
The average salt consumption and the relationship between daily salt consumption and BP in the Turkish population was evaluated recently by the SALTurk study, which was conducted with 1970 participants distributed throughout 14 cities across Turkey in 2008. According to the unpublished results of this study, an increase of 10 in the body mass index was determined to be associated with a 9.98 mm Hg increase in SBP and a 6.80 mm Hg increase in DBP, while an increase of 10 in age was associated with a 3.6 mm Hg increase in SBP and a 1.7 mm Hg increase in DBP. In addition, salt intake of 100 mEq per day (∼6 g salt) was associated with an 8.2 mm Hg increase in SBP and a 4.9 mm Hg increase in DBP.
In this regard, the most significant causes of not achieving TBP at the initial visit were stated to be non-compliance with dietary recommendations, patient-related factors and insufficient doses of antihypertensive medications. Accordingly, the main treatment plans that most investigators estimated would enable a TBP within 1–4 weeks included lifestyle recommendations, patient training and the addition of a new drug to the therapy. However, in contrast to the expectations, measures taken to reach TBP do not seem be effective because almost half of the patients are still far from the target levels defined in the guidelines at the end of 2 months. At that time, patient non-compliance and initially high BP levels were the main factors considered among the causes of failure.
Nevertheless, measures selected by the investigators to reach a TBP after visit 2 remained exactly the same as that of visit 1: lifestyle recommendations, patient training and the addition of a new drug to the therapy. Personal views that were shown to be more optimistic than the guidelines in TBP achievement rates may mistakenly lead investigators to believe that the ongoing treatment plans serve the purpose in the absence of more substantial and effective measures in the control of hypertension.
In fact, emphasizing patient-related factors seems reasonable as long as the clinician–patient partnership is based on trust and respect, and a holistic knowledge of the patient correlates with the positive outcomes of care, such as adherence, satisfaction and an improved health status.1 In addition to motivation, patients need specific education designed to help them modify their lifestyle and to take medications as prescribed to feel better and to reduce risks.1
Indeed, self-management of hypertension, in combination with the telemonitoring of BP measurements, was documented to represent an important new addition to the control of hypertension in primary care.11 In a past study examining the effects of a patient behavioral intervention delivered by telephone, home BP monitoring, and a combination of these interventions in improving BP among hypertensive adults treated in primary care (n=475) during a 24-month follow-up, no intervention alone was reported to improve BP control at 24 months, but the combination of interventions resulted in a clinically significant improvement in BP control of 11% compared with usual care.12
On the other hand, the clinician and the patient must agree on BP goals and an estimated achievement time, and the patient must be empowered with the understanding that making behavioral changes is ultimately his or her responsibility, rather than assigning the same intervention to every patient.1, 13
Mostly because of the difference in BP measurement devices used, a similar optimism was also evident in the BP levels measured at home by the patient because significantly higher levels were obtained in the cases of office records. Indeed, the decreased use of mercury in sphygmomanometers because of potential mercury spillage contaminating the environment, which has raised concerns regarding the accuracy of no mercury sphygmomanometers, has created new challenges for accurate BP determination.14 Therefore, it has been recommended that the replacement of mercury sphygmomanometers with new equipment must be on the basis of an appropriate validation and a regular check for accuracy, including all home BP measurement devices.1, 15
Data from observational studies and clinical trials suggest that poor SBP control, which is largely responsible for the unacceptably low rates of overall BP control,16, 17 is at least in part related to physician attitudes because most of them have been taught that the DBP is more important than the SBP, and thus treat accordingly. Fortunately, our physicians seem to recognize the importance of SBP control, based on their identification of a much larger patient population in cases of systolic rather than DBP (11.5% vs. 3.3%) that is far from the target levels.
The relationship between BP and the risk of cardiovascular events has been defined as continuous, consistent and independent of other risk factors. An increase in age was associated with an increased likelihood of myocardial infarction, peripheral vascular disease and concurrent revascularization in our patient population, whereas both age and DM were determined to significantly influence the prognosis. The relationship of older age to a better TBP achievement among female patients may be associated with the changing patterns of BP reported to occur with increasing age, including the continuous rise in SBP throughout the life in contrast to DBP.18, 19
The coexistence of hypertension in diabetes was documented to be particularly pernicious because of the increased risk of CVD, stroke, progression of renal disease and diabetic retinopathy.20 In addition, supporting the JNC-VI recommendation of <130/85 mm Hg for diabetic patients, the creatinine clearance in hypertensive type 2 diabetic patients may become stable over 5 years if BP is maintained at 132/78–138/86 mm Hg and if therapy is initiated before the onset of overt albuminuria.21 A recent ACCORD BP trial that evaluated the effect of targeting a SBP of 120 mm Hg compared with a goal of 140 mm Hg among patients with type 2 diabetes at high risk for cardiovascular events reported that lowering SBP from the mid-130s to approximately 120 mm Hg might not further reduce most cardiovascular events or the rate of death, and most of the benefit from lowering BP might be achieved by targeting a goal of <140 mm Hg.22 Notably, only a modest level of control of TBP was achieved among the patients with DM in the present study. Although evident in 16.2, 29.2 and 48.6% of the population, smoking, cardiovascular comorbidities and dyslipidemia were not determined to have a direct influence on the prognosis of hypertension in our population. Nevertheless, the management of these other risk factors is essential and should follow the established guidelines for controlling these coexisting problems that contribute to an overall cardiovascular risk.1
The prevalence of hypertension in Turkey was initially reported to be 30% by the TEKHARF study23 and was confirmed in 2004 to be 31.8% with the PatenT study,24 which was conducted with general practitioners. The data indicated that 32.2% of the PatenT study population had never had their BP measured. Overall, 40.7% of those with hypertension were aware of their diagnosis, but only 31.1% were receiving pharmacological treatment and only 8.1% had their BP under control. The subjects who were aware and treated had a control incidence of 20.7%, according to the PatenT study.24
In this respect, the introduction of new therapeutic agents and better patient compliance, as well as the inclusion of cardiologists and internal medicine specialists as investigators in the present study may have a role in the better control of hypertension observed compared with the PatenT study.
Nevertheless, the control rates in our population (SBP <140 mm Hg and DBP <90 mm Hg), although improved, are still far below the Healthy People goal of 50%, which was originally set as the year 2000 goal and has since been extended to 2010.1
Likewise, approximately 30% of adults were reported to be unaware of their hypertension, >40% of individuals with hypertension are not on treatment and two-thirds of hypertensive patients are not being controlled at BP levels <140/90 mm Hg in the USA.1
In conclusion, the results of this observational non-interventional study indicate that 29.5% of hypertensive patients who were enrolled in the study were under effective control and thus have reached their TBP levels according to the 2007 ESC/ESH criteria. When compared with the first visit, more patients achieved TBP levels specified by the 2007 ESC/ESH guidelines in the second visit. Investigators had a more optimistic perspective for their patients’ control of hypertension for both visits when compared with a data set analysis based on TBP levels defined in the 2007 ESC/ESH guidelines.
References
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, Jones DW, Materson BJ, Oparil S, Wright Jr JT, Roccella EJ . Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003; 42: 1206–1252.
World Health Report 2002. Reducing Risks, Promoting Healthy Life. World Health Organization: Geneva, Switzerland, 2002. http://www.who.int/whr/2002/en/.
Whelton PK . Epidemiology and the prevention of hypertension. J Clin Hypertension 2004; 6: 636–642.
Wolf-Maier K, Cooper RS, Kramer H, Banegas JR, Giampaoli S, Joffres MR, Poulter N, Primatesta P, Stegmayr B, Thamm M . Hypertension treatment and control in five European countries, Canada, and the United States. Hypertension 2004; 43: 10–17.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Struijker Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Kjeldsen SE, Erdine S, Narkiewicz K, Kiowski W, Agabiti-Rosei E, Ambrosioni E, Cifkova R, Dominiczak A, Fagard R, Heagerty AM, Laurent S, Lindholm LH, Mancia G, Manolis A, Nilsson PM, Redon J, Schmieder RE, Struijker-Boudier HA, Viigimaa M, Filippatos G, Adamopoulos S, Agabiti-Rosei E, Ambrosioni E, Bertomeu V, Clement D, Erdine S, Farsang C, Gaita D, Kiowski W, Lip G, Mallion JM, Manolis AJ, Nilsson PM, O’Brien E, Ponikowski P, Redon J, Ruschitzka F, Tamargo J, van Zwieten P, Viigimaa M, Waeber B, Williams B, Zamorano JL, The task force for the management of arterial hypertension of the European Society of Hypertension, The task force for the management of arterial hypertension of the European Society of Cardiology. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: 1462–1536.
Ong KL, Cheung BM, Man YB, Lau CP, Lam KS . Prevalence, awareness, treatment, and control of hypertension among United States adults 1999-2004. Hypertension 2007; 49: 69–75.
Redon J, Erdine S, Böhm M, Ferri C, Kolloch R, Kreutz R, Laurent S, Persu A, Schmieder RE . Physician attitudes to blood pressure control: findings from the Supporting Hypertension Awareness and Research Europe-wide survey. J Hypertens 2011; 29: 1633–1640.
Whelton PK, He J, Appel LJ, Cutler JA, Havas S, Kotchen TA, Roccella EJ, Stout R, Vallbona C, Winston MC, Karimbakas J . Primary prevention of hypertension: Clinical and public health advisory from The National High Blood Pressure Education Program. JAMA 2002; 288: 1882–1888.
Mancia G, Grassi G . Systolic and diastolic blood pressure control in antihypertensive drug trials. J Hypertens 2002; 20: 1461–1464.
Putnam W, Lawson B, Buhariwalla F, Goodfellow M, Goodine RA, Hall J, Lacey K, Macdonald I, Burge FI, Natarajan N, Sketris I, Mann B, Dunbar P, Van Aarsen K, Godwin MS . Hypertension and type 2 diabetes: What family physicians can do to improve control of blood pressure - an observational study. BMC Fam Pract 2011; 12: 86.
McManus RJ, Mant J, Bray EP, Holder R, Jones MI, Greenfield S, Kaambwa B, Banting M, Bryan S, Little P, Williams B, Hobbs FD . Telemonitoring and self-management in the control of hypertension (TASMINH2): a randomised controlled trial. Lancet 2010; 376: 163–172.
Bosworth HB, Olsen MK, Grubber JM, Neary AM, Orr MM, Powers BJ, Adams MB, Svetkey LP, Reed SD, Li Y, Dolor RJ, Oddone EZ . Two self-management interventions to improve hypertension control: a randomized trial. Ann Intern Med 2009; 151: 687–695.
Emmons KM, Rollnick S . Motivational interviewing in health care settings. Opportunities and limitations. Am J Prev Med 2001; 20: 68–74.
Jones DW, Appel LJ, Sheps SG, Roccella EJ, Lenfant C . Measuring blood pressure accurately: New and persistent challenges. JAMA 2003; 289: 1027–1030.
Canzanello VJ, Jensen PL, Schwartz GL . Are aneroid sphygmomanometers accurate in hospital and clinic settings? Arch Intern Med 2001; 161: 729–731.
Hyman DJ, Pavlik VN . Characteristics of patients with uncontrolled hypertension in the United States. N Engl J Med 2001; 345: 479–486.
Lloyd-Jones DM, Evans JC, Larson MG, O′Donnell CJ, Roccella EJ, Levy D . Differential control of systolic and diastolic blood pressure: Factors associated with lack of blood pressure control in the community. Hypertension 2000; 36: 594–599.
Burt VL, Whelton P, Roccella EJ, Brown C, Cutler JA, Higgins M, Horan MJ, Labarthe D . Prevalence of hypertension in the US adult population. Results from the Third National Health and Nutrition Examination Survey, 1988-1991. Hypertension 1995; 25: 305–313.
Franklin SS, Gustin W, Wong ND, Larson MG, Weber MA, Kannel WB, Levy D . Hemodynamic patterns of age-related changes in blood pressure. The Framingham Heart Study. Circulation 1997; 96: 308–315.
Kohner EM, Aldington SJ, Stratton IM, Manley SE, Holman RR, Matthews DR, Turner RC . United Kingdom prospective diabetes study, 30: diabetic retinopathy at diagnosis of non-insulin-dependent diabetes mellitus and associated risk factors. Arch Ophthalmol 1998; 116: 297–303.
Estacio RO, Jeffers BW, Gifford N, Schrier RW . Effect of blood pressure control on diabetic microvascular complications in patients with hypertension and type 2 diabetes. Diabetes Care 2000; 23 (Suppl 2): B54–B64.
ACCORD Study Group, Cushman WC, Evans GW, Byington RP, Goff Jr DC, Grimm Jr RH, Cutler JA, Simons-Morton DG, Basile JN, Corson MA, Probstfield JL, Katz L, Peterson KA, Friedewald WT, Buse JB, Bigger JT, Gerstein HC, Ismail-Beigi F . Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med 2010; 362: 1575–1585.
Onat A, Dursunoglu D, Sansoy V, Donmez K, Keles I, Okcun B, Kahraman G . Clinical Investigations Trends in Blood Pressure Levels in Turkish Adults: 5-year Follow-up of Original Cohort. Türk Kardiyol Dern Ars 1996; 24: 9–14.
Altun B, Arici M, Nergizog?lu G, Derici U, Karatan O, Turgan C, Sindel S, Erbay B, Hasanoǧlu E, Caǧlar S . Prevalence, awareness, treatment and control of hypertension in Turkey (the PatenT study) in 2003. J Hypertens 2005; 23: 1817–1823.
Acknowledgements
The study was funded by Sanofi-Aventis Turkey. We thank Cagla Isman, M.D. and Professor Sule Oktay, M.D., Ph.D. from KAPPA Consultancy Traning Research Ltd., Istanbul, who provided editorial support; and Oguz Akbas, M.D., Ph.D., Esra Koruyucu and Arzu Çalιşgan M. Sc. from Monitor CRO, Istanbul, for their support of the statistical analysis, funded by Sanofi-Aventis Turkey.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
The members of i-target Goal Study are mentioned in Appendix.
Appendix
Appendix
i-Target Study Group (by the center's name in descending order of number of patients enrolled) Prof. Saide Aytekin, MD; Bilim University, Faculty of Medicine, Istanbul (Study Coordinator); A. Oǧuz Baktιr, MD; Antalya State Hospital, Antalya; Assist. Prof. Ahmet Akçay, MD; Sutcu Imam University, Faculty of Medicine, Maras; Ahmet Akιn, MD; Kartal Training and Research Hospital, Istanbul; Ahmet Karabulut, MD; Private Medicine Hospital, Istanbul; Prof. Ali Aydιnlar, MD; Uludaǧ University, Faculty of Medicine, Bursa; Ali Köse, MD; Kayseri Ibn-i Sina Hospital, Kayseri; Assoc. Prof. Alparslan Birdane, MD; Osmangazi University, Faculty of Medicine, Eskisehir; Alpay Onuk, MD; Kayseri Geriatrics Center, Kayseri; Arif Yücel, MD; Private Sifa Hospital, Yozgat; Assoc. Prof. Atila Bitigen, MD; Private Medical Park Hospital, Istanbul; Atilla Soyelcin, MD; Private Clinic, Eskisehir; Aydιn Ünsal, MD; Gölcük Medical Center, Kocaeli; Ayhan Tan, MD; Eyüp State Hospital, Istanbul; Assoc. Prof. Aziz Karadede, MD; Dicle University, Faculty of Medicine, Diyarbakir; Baki Ozsoy, MD; Kayseri Training and Research Hospital, Kayseri; Bekir Kalaycι, MD; Private Park Afyon Hospital; Afyon; Beste Ozben, MD; Marmara University, Faculty of Medicine, Istanbul; Beyhan Tiryaki, MD; Gaziantep Private Sani Konukoǧlu Hospital, Gaziantep; Birgül Özgül, MD; Kesan State Hospital, Kesan; Birtan Acay, MD; Private Kanarya Anadolu Policlinic, Istanbul; Bülent Eralp, MD; Goztepe Training and Research Hospital; Istanbul; Celal Kιrdar, MD; Eskisehir State Hospital, Eskisehir; Assist. Prof. Cihan Dündar, MD; Kartal Kosuyolu Yuksek Ihtisas Hospital, Istanbul; Dilek Soysal, MD; Izmir Ataturk Training and Research Hospital, Izmir; Doǧu Kιlιç, MD; Pamukkale University, Faculty of Medicine, Denizli; Ebru Ozpelit, MD; Dokuz Eylül University, Faculty of Medicine, Izmir; Ekrem Cakir, MD; Sakarya Training and Research Hospital, Adapazari; Emrah Gunay, MD; Ankara Numune Training and Research Hospital, Ankara; Ender Ucar, MD; Gemlik State Hospital; Bursa; Enver Eroglu, MD; Tosya State Hospital, Kastamonu; Erol Aslan, MD; Private Mujde Hospital, Malatya; Assoc. Prof. Ersel Onrat, MD; Kocatepe University, Faculty of Medicine, Afyon; Ertugrul Okuyan, MD; Bagcilar State Hospital, Istanbul; Assist. Prof. Faruk Ayan, MD; Cerrahpasa University, Faculty of Medicine, Istanbul; Prof. Ferhan Candan, MD; Cumhuriyet University, Faculty of Medicine; Sivas; Feridun Ozdemir, MD; Aksaray Heart Center, Aksaray; Figen Cagilci, MD; Trabzon Numune Hospital, Trabzon; Prof. Filiz Ozerkan, MD; Ege University, Faculty of Medicine, Izmir; Assoc. Prof. Guliz Kozdag, MD; Kocaeli University, Faculty of Medicine, Kocaeli; Prof. H. Huseyin Telli, MD; Selçuk University, Faculty of Medicine, Konya; Hadi Selimoglu, MD; Malatya State Hospital, Malatya; Halil Rakici, MD; Rize 82. Yil State Hospital, Rize; Halil Uzuner, MD; Odemis State Hospital, Izmir; Haluk Tan, MD; Tarsus Private Umut Medical Center, Mersin; Hasan Ari, MD; Bursa Yuksek Ihtisas Training and Research Hospital, Bursa; Havva Cilan, MD; Av. Cengiz Gokcek State Hospital, Gaziantep; Ibrahim Duman, MD; Aksehir State Hospital, Konya; Imran Onur, MD; Bagcilar State Hospital, Istanbul; Iskender Yüksel, MD; Sinop Ayancik State Hospital, Sinop; Ismail Biyik, MD; Usak State Hospital, Usak; Assist. Prof. Ismet Durmus, MD; Karadeniz Teknik University, Faculty of Medicine, Trabzon; Prof. Izzet Tandoǧan, MD; Cumhuriyet University, Faculty of Medicine, Sivas; Assist. Prof. Kenan Durna, MD; Private Mediva Hospital, Samsun; Assist. Prof. Kenan Iltumur, MD; Dicle University, Faculty of Medicine, Diyarbakir; Levent Sarac, MD; Istinye State Hospital, Istanbul; M. Hakan Öncel, MD; Sanliurfa Balikligol State Hospital, Sanliurfa; M. Akif Uzun, MD; Samsun Gazi State Hospital, Samsun; M.Emin Dincag, MD; Private Akademi Medical Center, Samsun; M.Yunus Emiroglu, MD; Pasabahce State Hospital, Istanbul; Meftun Celikci, MD; Private Medical Park Hospital, Batman; Prof. Mehmet Agirbasli, MD; Marmara University, Faculty of Medicine, Istanbul; Mehmet Ali Kosekli, MD; Denizli State Hospital, Denizli; Mehmet Bulbul, MD; Burdur State Hospital, Burdur; Assoc. Prof. Mesut Demir, MD; Cukurova University, Faculty of Medicine, Adana; Muazzez Caymaz, MD; Private Iskenderun Deniz Medical Center, Iskenderun; Murat Gulener, MD; Anamur State Hospital, Anamur; Mustafa Bozkurt, MD; Vakif Gureba Training and Research Hospital, Istanbul; Assist. Prof. Mustafa Ozturk, MD; Van 100. Yil University, Faculty of Medicine, Van; Mustafa Soyturk, MD; Antalya State Hospital, Antalya; Mustafa Togan, MD; Konya Eregli State Hospital, Konya; Assoc. Prof. Mustafa Tuncer, MD; Van 100. Yil University, Faculty of Medicine, Van; Mustafa Turgut, MD; Aksaray State Hospital, Aksaray; Nazmi Ilker Bayrak, Iskenderun State Hospital, Iskenderun; Assoc. Prof. Nese Cam, MD; Siyami Ersek Tarining and Researh Hospital, Istanbul; Omer Incecayir, MD; Yozgat State Hospital, Yozgat; Oner Ozdogan, MD; Tepecik State Hospital, Izmir; Assist. Prof. Ozan Utuk, MD; Celal Bayar University, Faculty of Medicine, Manisa; Pervin Baysal, MD; Private Atasam Hospital, Samsun; Assist. Prof. Ramazan Esen, MD; Van Ipekyolu State Hospital, Van; Recep Yoldas, MD; Konya Numune Hospital, Konya; Sait Onal, MD; Private Selcuklu Hospital, Konya; Sami Ayhan, MD; Karasu State Hospital, Kocaeli; Sedat Yuksel, MD; Konya Numune Hospital, Konya; Prof. Sema Guneri, MD; Dokuz Eylul University, Faculty of Medicine, Izmir; Assist. Prof. Serhat Icagasioglu, MD; Cumhuriyet University, Faculty of Medicine, Sivas; Sevda Yilmaz Erener, MD; Esenyurt State Hospital, Istanbul; Seyhmus Akapoglu, MD; Mardin State Hospital, Mardin; Taha Okan, MD; Private Kardiya Medical Center, Izmir; Prof. Taner Akdere, MD; Unye State Hospital, Ordu; Taner Cavusoglu, MD; Duzce Ataturk State Hospital, Bolu; Assist. Prof. Turker Tasliyurt, MD; Gaziosmanpasa University, Faculty of Medicine, Tokat; Ugur Coskun, MD; Surp Pirgic Ermeni Hospital, Istanbul; Ugur Ozensoy, MD; Izmit Seka State Hospital, Kocaeli; Yasar Sertbas, MD; Uskudar State Hospital, Istanbul; Yuksel Aksoy, MD; Private Bayindir Hospital, Ankara; Assist. Prof. Zafer Elbasan, MD; Nigde State Hospital, Nigde; Zeki Dogan, MD; Private Medical Park Hospital, Batman; Prof. Zerrin Yigit, MD; Istanbul University Cardiology Institute, Istanbul.
Rights and permissions
About this article
Cite this article
Aytekin, S., Guneri, S., Cam, N. et al. An observational study to evaluate factors responsible and actions taken for hypertensive patients who are not at blood pressure goal: i-target Goal Study. Hypertens Res 35, 624–632 (2012). https://doi.org/10.1038/hr.2012.12
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2012.12
Keywords
This article is cited by
-
Arterial hypertension assessed “out-of-office” in a contemporary cohort of rheumatoid arthritis patients free of cardiovascular disease is characterized by high prevalence, low awareness, poor control and increased vascular damage-associated “white coat” phenomenon
Arthritis Research & Therapy (2013)
