
The Epidemiologic Transition in French Guiana: Secular Trends and Setbacks, and Comparisons with Continental France and South American Countries

 ,
,  , , and
, , and 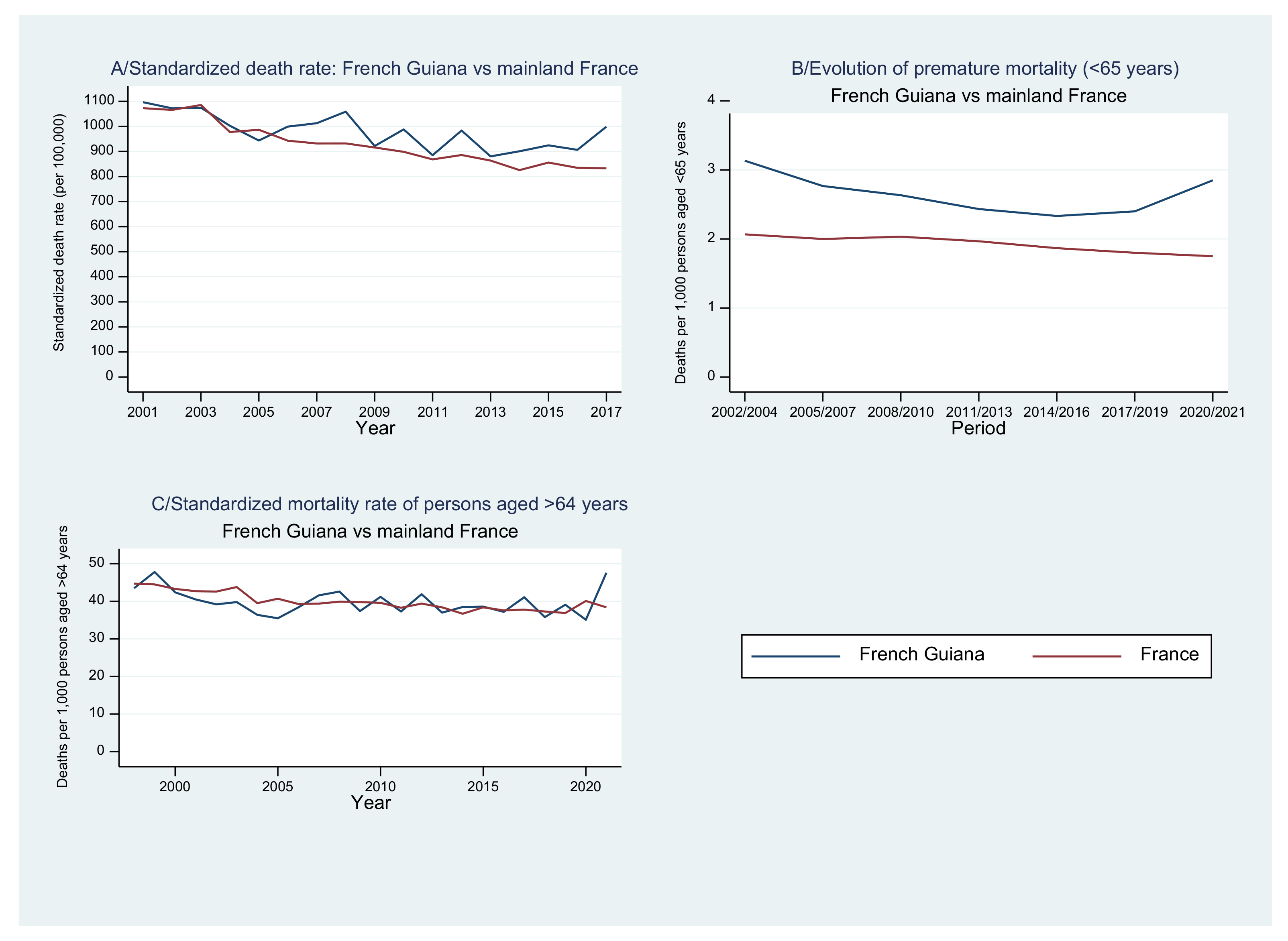{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Results
3.1. Mortality Statistics
3.2. Evolution of the Standardized Death Rate, Premature Mortality, and over 64 Mortality
3.3. Evolution of Under-5 Mortality
3.4. Main Causes of Early Death
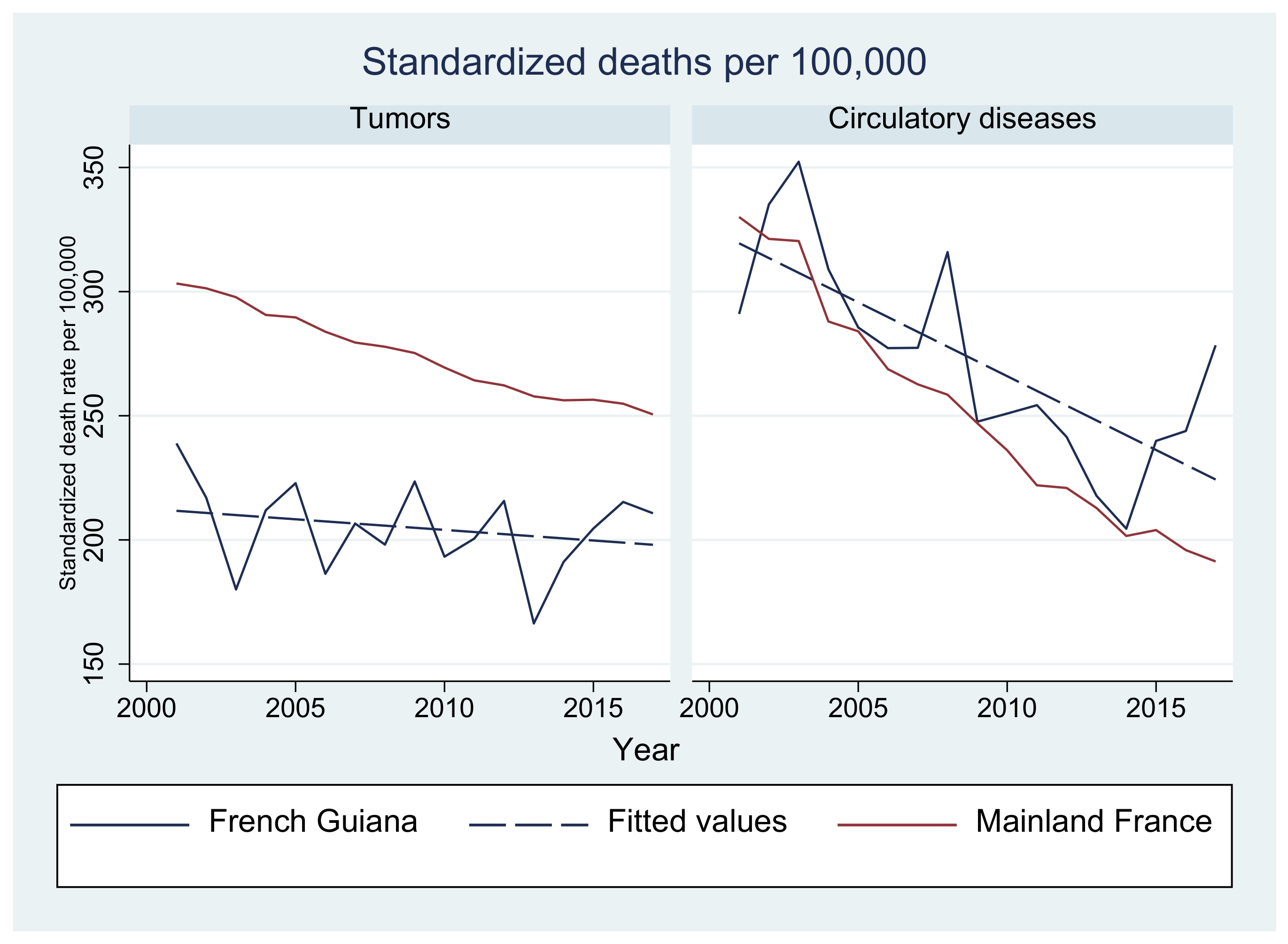
3.5. Evolution of the Main Causes of Death
3.6. Evolution of Infections as a Cause of Premature Death
3.7. Life Expectancy
3.7.1. Life Expectancy at Birth
3.7.2. Life Expectancy at 20, 40, and 60 Years
3.7.3. Gains
3.7.4. Population Growth and Structure
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McKeown, R.E. The Epidemiologic Transition: Changing Patterns of Mortality and Population Dynamics. Am. J. Lifestyle Med. 2009, 3, 19S–26S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santosa, A.; Wall, S.; Fottrell, E.; Högberg, U.; Byass, P. The Development and Experience of Epidemiological Transition Theory over Four Decades: A Systematic Review. Glob. Health Action 2014, 7, 23574. [Google Scholar] [CrossRef] [PubMed]
- Zéphirin, R. Political Demography and Urban Governance in French Guyana: Implications for Latin America and the Caribbean; Springer: Singapore, 2020; ISBN 9789811538315. [Google Scholar]
- Van Melle, A.; Cropet, C.; Parriault, M.-C.; Adriouch, L.; Lamaison, H.; Sasson, F.; Duplan, H.; Richard, J.-B.; Nacher, M. Renouncing Care in French Guiana: The National Health Barometer Survey. BMC Health Serv. Res. 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Available online: https://ourworldindata.org (accessed on 15 November 2022).
- Dossier Complet—Département de La Guyane (973) | Insee. Available online: https://www.insee.fr/fr/statistiques/2011101?geo=DEP-973 (accessed on 15 November 2022).
- Article-Bulletin Épidémiologique Hebdomadaire. Available online: http://beh.santepubliquefrance.fr/beh/2020/2-3/2020_2-3_1.html (accessed on 16 November 2022).
- De Thoisy, B.; Duron, O.; Epelboin, L.; Musset, L.; Quénel, P.; Roche, B.; Binetruy, F.; Briolant, S.; Carvalho, L.; Chavy, A.; et al. Ecology, Evolution, and Epidemiology of Zoonotic and Vector-Borne Infectious Diseases in French Guiana: Transdisciplinarity Does Matter to Tackle New Emerging Threats. Infect. Genet. Evol. 2021, 93, 104916. [Google Scholar] [CrossRef] [PubMed]
- Interroger Les Données de Mortalité | CépiDc. Available online: https://www.cepidc.inserm.fr/causes-medicales-de-deces/interroger-les-donnees-de-mortalite (accessed on 15 November 2022).
- SPF La Mortalité “Evitable” Liée Aux Comportements à Risque, Une Priorité de Santé Publique en France. Numéro Thématique. La Mortalité Prématurée en France. Available online: https://www.santepubliquefrance.fr/notices/la-mortalite-evitable-liee-aux-comportements-a-risque-une-priorite-de-sante-publique-en-france.-numero-thematique.-la-mortalite-prematuree-en-fr (accessed on 2 February 2023).
- Leneuve-Dorilas, M.; Favre, A.; Carles, G.; Louis, A.; Nacher, M. Risk Factors for Premature Birth in French Guiana: The Importance of Reducing Health Inequalities. J. Matern. -Fetal Neonatal Med. 2019, 32, 1388–1396. [Google Scholar] [CrossRef] [PubMed]
- Nacher, M.; Lambert, V.; Favre, A.; Carles, G.; Elenga, N. High Mortality Due to Congenital Malformations in Children Aged < 1 Year in French Guiana. BMC Pediatr. 2018, 18, 393. [Google Scholar] [CrossRef] [Green Version]
- Le Plan Blanc Déclenché au CHOG: Le Nombre de Patientes en Service Maternité Explose. Available online: https://la1ere.francetvinfo.fr/guyane/ouest-guyanais/saint-laurent-du-maroni/le-plan-blanc-declenche-au-chog-le-nombre-de-patientes-en-service-maternite-explose-893502.html (accessed on 5 April 2023).
- Imounga, L.M.; Plenet, J.; Belliardo, S.; Chine, E.C.; Louvel, D.; Cenciu, B.; Couppié, P.; Alsibai, K.D.; Nacher, M. Gastric Cancer Incidence and Mortality in French Guiana: South American or French? J. Gastrointest. Cancer 2022, 53, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Imounga, L.M.; Plenet, J.; Belliardo, S.; Chine, E.C.; Adenis, A.; Gaillet, M.; Thomas, N.; Michaud, C.; Servas, V.; Couppié, P.; et al. Incidence and Mortality of Cervical Cancer in French Guiana: Temporal and Spatial Trends. Public Health Pract. 2021, 2, 100138. [Google Scholar] [CrossRef] [PubMed]
- Article-Bulletin Épidémiologique Hebdomadaire. Available online: http://beh.santepubliquefrance.fr/beh/2020/36-37/2020_36-37_5.html (accessed on 18 November 2022).
- Question N°2260-Assemblée Nationale. Available online: https://questions.assemblee-nationale.fr/q15/15-2260QG.htm (accessed on 16 November 2022).
- « Cet Hôpital Est un Mouroir ». Available online: https://www.guadeloupe.franceantilles.fr/cet-hopital-est-un-mouroir-753184.php (accessed on 16 November 2022).
- Massicard, M.; Drak Alsibai, K.; Nacher, M.; Sabbah, N. Nutritional and Socioeconomic Determinants of Overweight and Obesity in the French Amazon: The Health Barometer Study. Front. Endocrinol 2022, 13, 849718. [Google Scholar] [CrossRef]
- Un Tiers Des Guyanais Ont Retardé Ou Renoncé à Un Soin Médical En 2019-Insee Analyses Guyane-52. Available online: https://www.insee.fr/fr/statistiques/5391092 (accessed on 16 November 2022).
- VaccinTracker Covid19: Nombre de Français Vaccinés. CovidTracker. Available online: https://covidtracker.fr/vaccintracker/ (accessed on 16 November 2022).
- Conan, C. Les Populations Aux Frontières de La Guyane: Caractéristiques Singulières et Fécondités Contrastées: Une Recherche Menée Dans Les Communes Guyanaises de Maripasoula, Grand-Santi, Saint-Laurent-Du-Maroni, Mana et Saint-Georges de l’Oyapock, Ainsi Que Dans Le Municipio d’Oiapoque (Brésil). Ph.D. Thesis, Universite Pantheon-Sorbonne-Paris I, Paris, France, 2018. [Google Scholar]
- Poursuite de La Transition Démographique En Guyane-Légère Inflexion de La Natalité-Insee Analyses Guyane-12. Available online: https://www.insee.fr/fr/statistiques/1908375 (accessed on 16 November 2022).
- McCracken, K.; Phillips, D.R. Demographic and Epidemiological Transition. In International Encyclopedia of Geography; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2017; pp. 1–8. ISBN 978-1-118-78635-2. [Google Scholar]
- Hallet, E.; Flamand, C.; Rousset, D.; Bonifay, T.; Fritzell, C.; Matheus, S.; Dueymes, M.; Ntab, B.; Nacher, M. ZIKA Virus Infection in Pregnant Women in French Guiana: More Precarious-More at Risk. PLoS Negl. Trop. Dis. 2020, 14, e0008193. [Google Scholar] [CrossRef] [PubMed]
- Rochemont, D.R.; Mimeau, E.; Misslin, C.; Papaix-Puech, M.; De Toffol, B.; Sabbah, N.; Delmas, E.; Bejot, Y.; Fournel, I.; Nacher, M. A Prospective Comparative Study of Health Inequalities and the Epidemiology of Stroke in French Guiana and Dijon, France. Front. Public Health 2022, 10, 849036. [Google Scholar] [CrossRef] [PubMed]
- Rochemont, D.R.; Lemenager, P.; Franck, Y.; Farhasmane, A.; Sabbah, N.; Nacher, M. The Epidemiology of Acute Coronary Syndromes in French Guiana. In Proceedings of the Annales de Cardiologie et d’Angéiologie; Elsevier: Hoboken, NJ, USA, 2021; Volume 70, pp. 7–12. [Google Scholar]
- La Guyane, Une Région Jeune et Cosmopolite-Insee Analyses Guyane-35. Available online: https://www.insee.fr/fr/statistiques/3695893 (accessed on 12 January 2023).









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nacher, M.; Basurko, C.; Douine, M.; Lambert, Y.; Hcini, N.; Elenga, N.; Le Turnier, P.; Epelboin, L.; Djossou, F.; Couppié, P.; et al. The Epidemiologic Transition in French Guiana: Secular Trends and Setbacks, and Comparisons with Continental France and South American Countries. Trop. Med. Infect. Dis. 2023, 8, 219. https://doi.org/10.3390/tropicalmed8040219
Nacher M, Basurko C, Douine M, Lambert Y, Hcini N, Elenga N, Le Turnier P, Epelboin L, Djossou F, Couppié P, et al. The Epidemiologic Transition in French Guiana: Secular Trends and Setbacks, and Comparisons with Continental France and South American Countries. Tropical Medicine and Infectious Disease. 2023; 8(4):219. https://doi.org/10.3390/tropicalmed8040219
Chicago/Turabian StyleNacher, Mathieu, Célia Basurko, Maylis Douine, Yann Lambert, Najeh Hcini, Narcisse Elenga, Paul Le Turnier, Loïc Epelboin, Félix Djossou, Pierre Couppié, and et al. 2023. "The Epidemiologic Transition in French Guiana: Secular Trends and Setbacks, and Comparisons with Continental France and South American Countries" Tropical Medicine and Infectious Disease 8, no. 4: 219. https://doi.org/10.3390/tropicalmed8040219